Crb 65 Score 0 / Validation Of The Qsofa Score Compared To The Crb 65 Score For Risk Prediction In Community Acquired Pneumonia Clinical Microbiology And Infection
CURB-65 or alternatively CRB-65. Method Medline 1966 to June 2009 Embase 1988 to November.

Platelet Counts In Relation To Crb 65 And Ps Index Scores Of 95 Cap Download Table
It uses low systolic BP S and poor oxygenation PaO2.

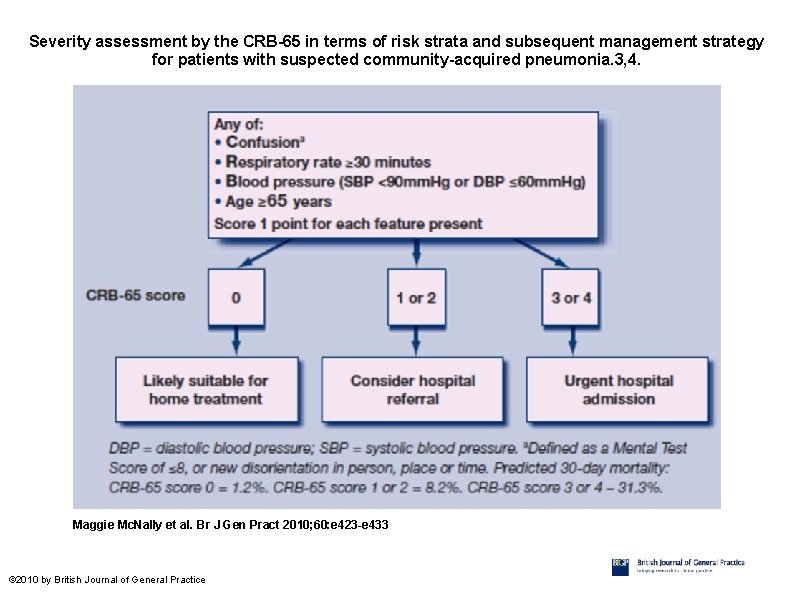
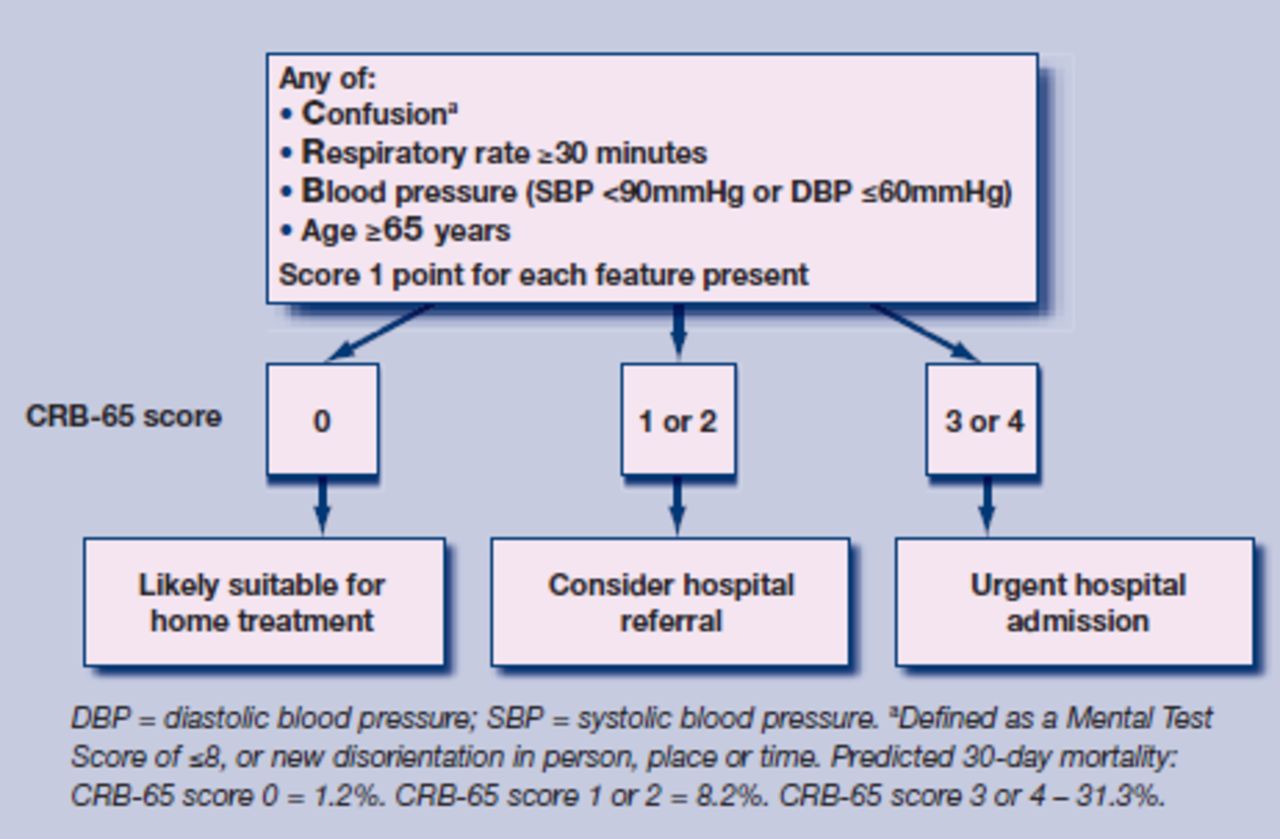
Crb 65 score 0. Diastolic pressure 60. Given that the CRB-65 is easier to handle we favour the use. 65 years of age or older patients who have a CRB65 score of 0 are at low risk of death and do not normally require hospitalisation for clinical reasons patients who have a CRB65 score of 1 or 2 are at increased risk of death particularly with a score of 2 and hospital referral and assessment should be.
It estimates mortality of community-acquired pneumonia and can help guide decision for inpatient vs outpatient management. Blood pressure systolic 65 years. FIO2 O advancing age A high respiratory rate R.
Aim The study sought to validate CRB-65 and assess its clinical value in community and hospital settings. Patients who have a CRB65 score of 0 are at low risk of death and do not normally require hospitalisation for clinical reasons patients who have a CRB65 score of 1 or 2 are at increased risk of death particularly with a score of 2 and hospital referral. Systolic BP 90 mmHg or Diastolic BP 60 mmHg 65 years of age.
Confusion abbreviated Mental Test score 8 or less or new disorientation in person place or time. Respiratory rate 30 breathsmin. With a CRB-65 score 0 32 3761172 of all patients were classified as at low risk.
The score can also be used to predict 30-day mortality. For guidance on delirium see the NICE guideline on delirium. CURB-65CRB-65 Score for Pneumonia Decision rules to help determine outpatient vs.
The CURB-score predicted 30-day mortality and critical pneumonia equally to the CRB-65 score with an AUC of 077 and 078 respectively. The corresponding values for the CURB-65 score were 081 and 079 which was a superior to the CRB65 score p 0001. A CRB-65 score can be calculated by omitting the blood urea nitrogen value which gives it a point range from 0 to 4.
Usually does not require hospitalization. The main use of the CURB-65 score is to predict the action needed to be taken for a patient with pneumonia. The main use of the CURB-65 score is to predict the action needed to be taken for a patient with pneumonia.
CURB-65 also known as the CURB criteria is a clinical prediction rule that has been validated for predicting mortality in community-acquired pneumonia and infection of any site. BUN 19 mgdL 7 mmolL Respiratory Rate 30 BP. Using the DS CRB-65 score 01 as a definition of low risk 51 5961172 of all patients would be included of whom two patients died.
Increased risk of death. Mortality rate 05. Inpatient treatment for pneumonia.
A modified version of the score known as CRB-65 is often performed in general practice to assess the need for. Immediate admission in ICU consider intensive care with score 4 to 5. The CURB-65 Score includes points for confusion and blood urea nitrogen which in the acutely ill elderly patient could be due to a variety of factors.
Here are the main actions. Thus if the patient needed supplemental oxygen when transported by ambulance before arrival at the ED the SpO 2 measured by the crew. The CRB-65-score is a clinical score that is used to roughly estimate the severity of community-acquired pneumoniasThe score corresponds to the statistical probability of patients dying because of pneumonia.
Prognostic scores The CRB-65 score was calculated according to the ori-ginal publication9 The lowest SpO 2 recorded either by the ambulance crew or at the ED was used when the DS CRB-65 score was calculated. Availability of the CRB-65 score 90 was far superior to that of CURB 65 due to missing blood urea nitrogen values P 0001. It was developed in 2002 at the University of Nottingham by Dr.
90 mmHg 1 Alder 65 år 1 I almen praksis udelades carbamidmåling CRB-65. BUN 19 is almost 20 for easy memorization. If cortisol was added further significant improvement of prediction resulted for both.
Confusion mental test score 8 new disorientation in person place or time BUN 20 mgdL. 30min Blood pressure. Interpreting the CURB-65 score.
Diagnose as an outpatient 0-1. The CURB-65 is based on the earlier CURB score and is recommended by the British Thoracic Society for the assessment of severity of pneumonia. Crb 65 score mdcalc.
Mortality rate 51 percentscore9CRB-65 0. Scores of 2 require more assistance and might need hospital admission and. This score is useful when blood tests are not read- ily available.
Interpretation of CURB-65 score. Both the CURB and CRB-65 scores can be used in the hospital and out-patients setting to assess pneumonia severity and the risk of death. Among these patients only one patient died.
Background The CRB-65 score is a clinical prediction rule that grades the severity of community-acquired pneumonia in terms of 30-day mortality. Recently Rate of respiration. In the case of cumulative scores of 0 or 1 outpatient treatment is advisable as the mortality risk is less than 3 in 30 days.
Medscape CURB-65 Calculator MDCALC CURB-65 Calculator AAFP CURB-65. Score 1 point for each of following features that are present. Rate 51 percentscore10CRB-65 1.
Treatments depend on the score and there are usually local hospital guidelines to follow. The following criteria are used to score the CRB-65. An alternative scoring system SOAR circumvents those two parameters.
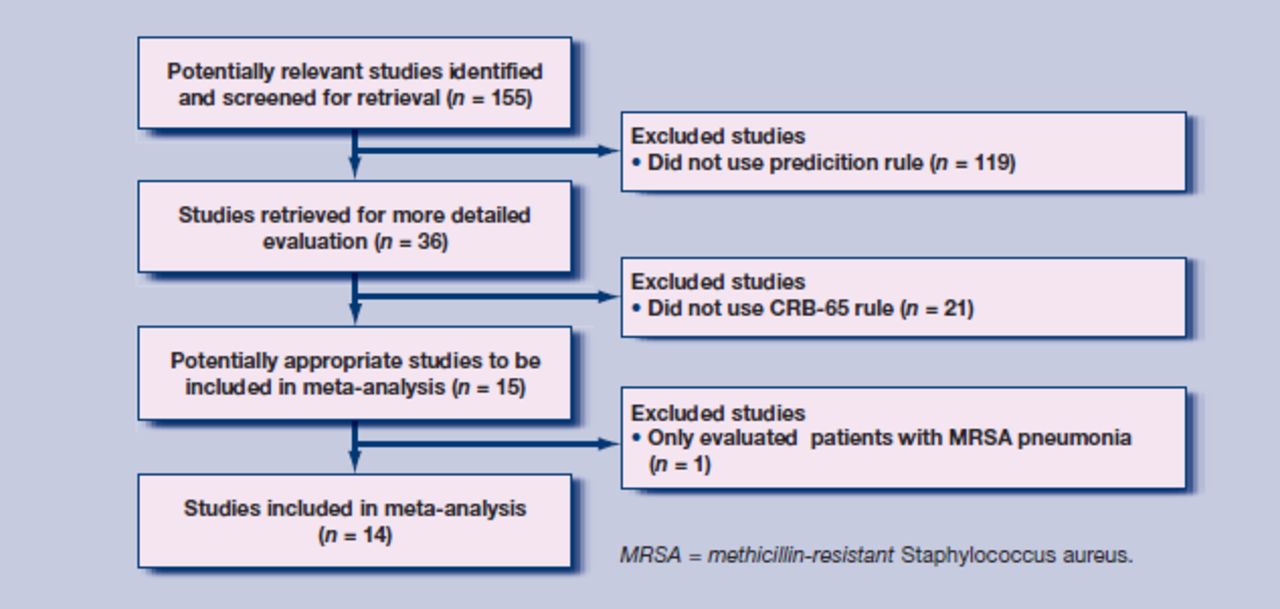
Raised respiratory rate 30 breaths per minute or more low blood pressure diastolic 60 mmHg or less or systolic less than 90 mmHg age 65. Design of study Systematic review and meta-analysis of validation studies of CRB-65. The overall CURB-65 score therefore ranges between 0 meaning no risk pneumonia if diagnosed and 5 which is indicative of very severe pneumonia.
Very low risk of death.
Https Www Aafp Org Fpm 2006 0400 Fpm20060400p41 Rt2 Pdf

Validation Of The Qsofa Score Compared To The Crb 65 Score For Risk Prediction In Community Acquired Pneumonia Clinical Microbiology And Infection
Determining Need For Hospitalisation Evaluation Of The Utility Of The Crb 65 Score In Patients With Community Acquired Pneumonia Presenting To An Emergency Department


Curb 65 Score Almostadoctor

Ps Index And Crb 65 Scores In Relation To In Hospital Mortality Of 95 Download Table

Defining Community Acquired Pneumonia Severity On Presentation To Hospital An International Derivation And Validation Study Thorax
Validity Of British Thoracic Society Guidance The Crb65
Systolic Blood Pressure Below 90mmhg And Assessment Of Covid 19 Severity With Crb 65 Score The New Neander S Medical

Continuous Variables Of Curb65 And Crb65 Scores With The Following Download Scientific Diagram

The Use Of The Crb 65 Severity Of Illness Score To Determine The Need For Admission Of Patients With Community Acquired Pneumonia Presenting To An Emergency Department Semantic Scholar

Validity Of British Thoracic Society Guidance The Crb 65 Rule For Predicting The Severity Of Pneumonia In General Practice Systematic Review And Meta Analysis British Journal Of General Practice

Modifications Of The Curb65 And Crb65 Scores For Prediction Of 30 Day Download Table
Validity Of British Thoracic Society Guidance The Crb 65 Rule For Predicting The Severity Of Pneumonia In General Practice Systematic Review And Meta Analysis British Journal Of General Practice

The Usefulness Of Confusion Urea Respiratory Rate And Shock Index Or Adjusted Shock Index Criteria In Predicting Combined Mortality And Or Icu Admission Compared To Curb 65 In Community Acquired Pneumonia

Figure 1 From Validity Of British Thoracic Society Guidance The Crb 65 Rule For Predicting The Severity Of Pneumonia In General Practice Systematic Review And Meta Analysis Semantic Scholar

The Use Of The Crb 65 Severity Of Illness Score To Determine The Need For Admission Of Patients With Community Acquired Pneumonia Presenting To An Emergency Department Semantic Scholar
Community Acquired Pneumonia

Validity Of British Thoracic Society Guidance The Crb 65 Rule For Predicting The Severity Of Pneumonia In General Practice Systematic Review And Meta Analysis British Journal Of General Practice

Outpatient Vs Inpatient Treatment Of Community Acquired Pneumonia Fpm